‘Don’t slouch!’ About the sideways spine curve and posture defects.
Does my child have scoliosis?
Scoliosis is a three-dimensional spine curve that usually occurs during adolescence, puberty and rapid growth. Infantile and toddler varieties are definitely less common.
80% of scoliosis is idiopathic, so we don’t know why they arise. Structural scoliosis affects 2-3% of children.
Is every torso asymmetry a scoliosis?
No. Most of the lateral curvatures, asymmetry of the position of the shoulders, shoulder blades, protruding shoulder blades, asymmetry of the waist cut and excessive humping are defects of posture. Postural defects, unlike scoliosis, are corrective, so we can influence them by tightening the appropriate muscle groups, correcting our own figure in front of the mirror. Postural defects affect the majority of society of all ages.

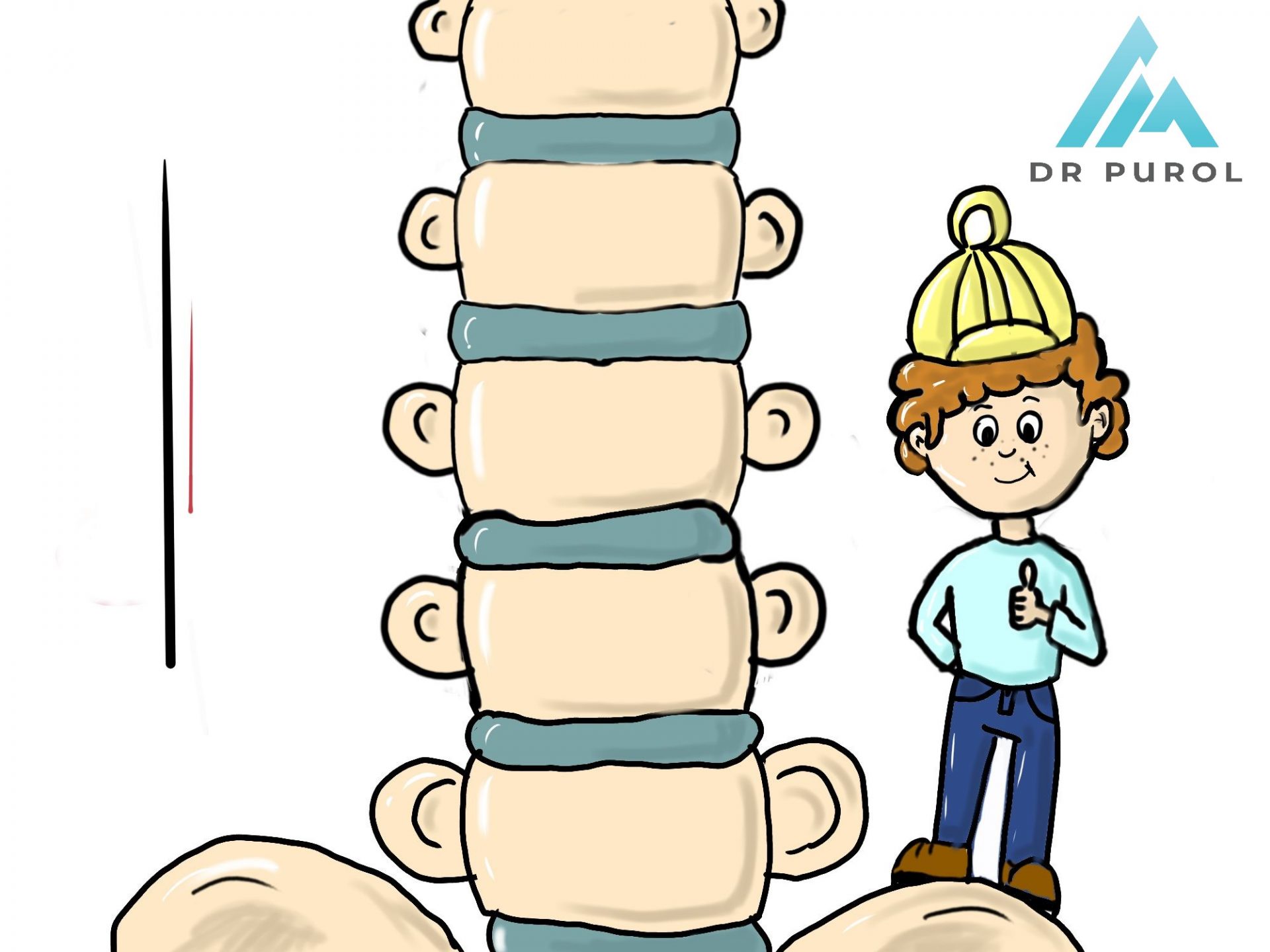
Scoliosis is a three-dimensional deformation that causes:
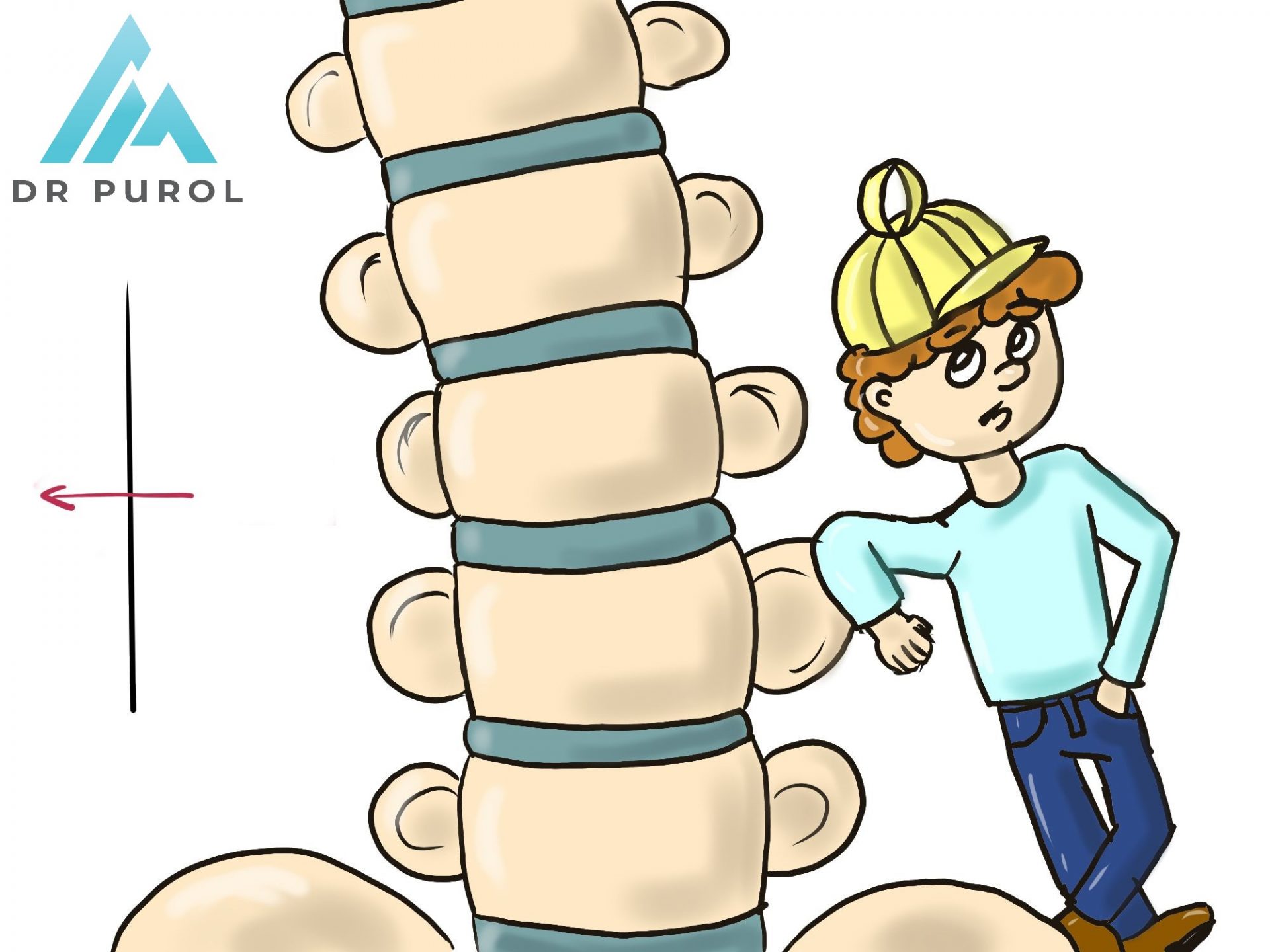
- lateral curvature of the spine in the frontal plane,
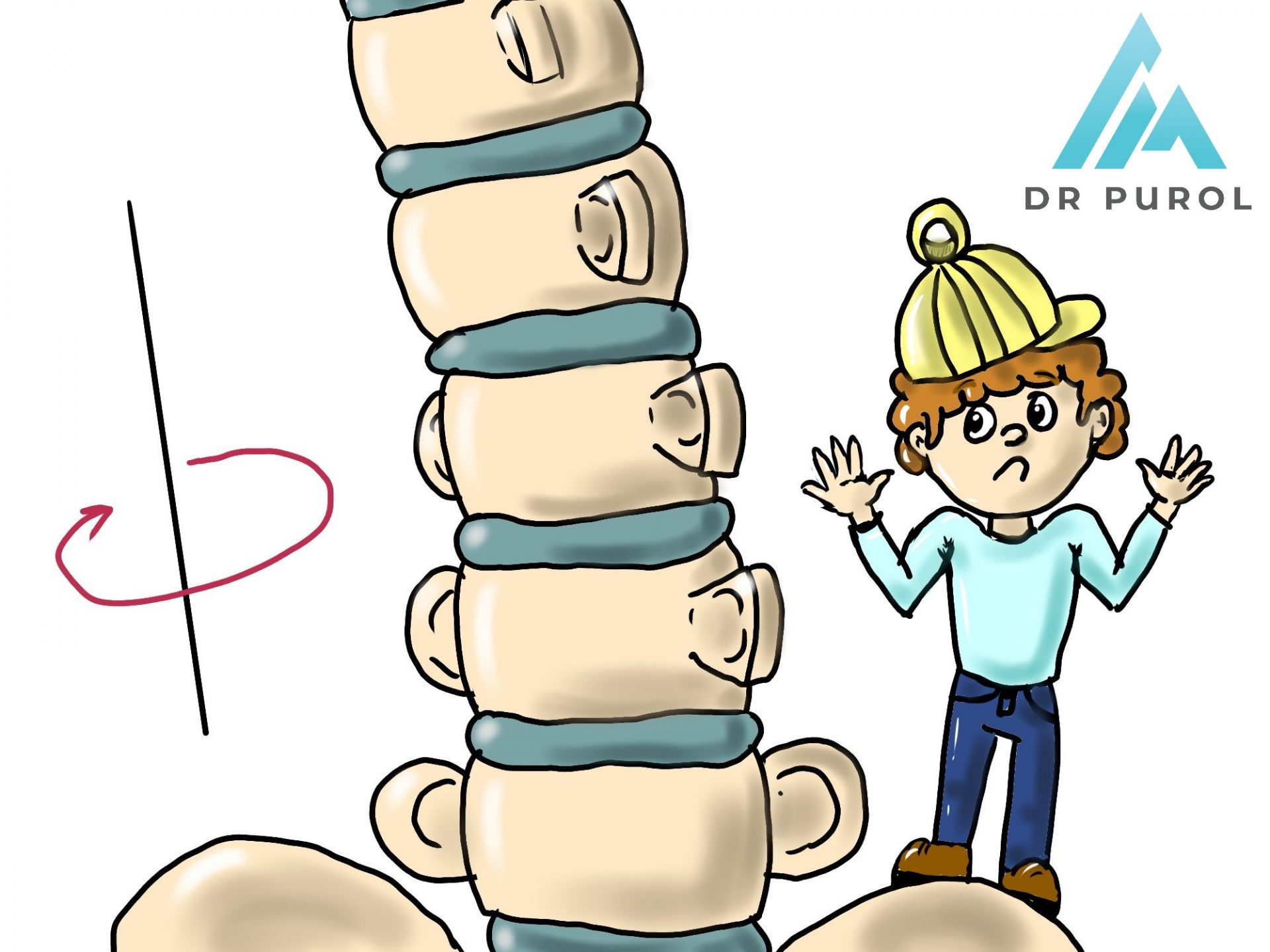
- rotation of the vertebrae with the formation of a costal hump or lumbar shaft in the horizontal plane
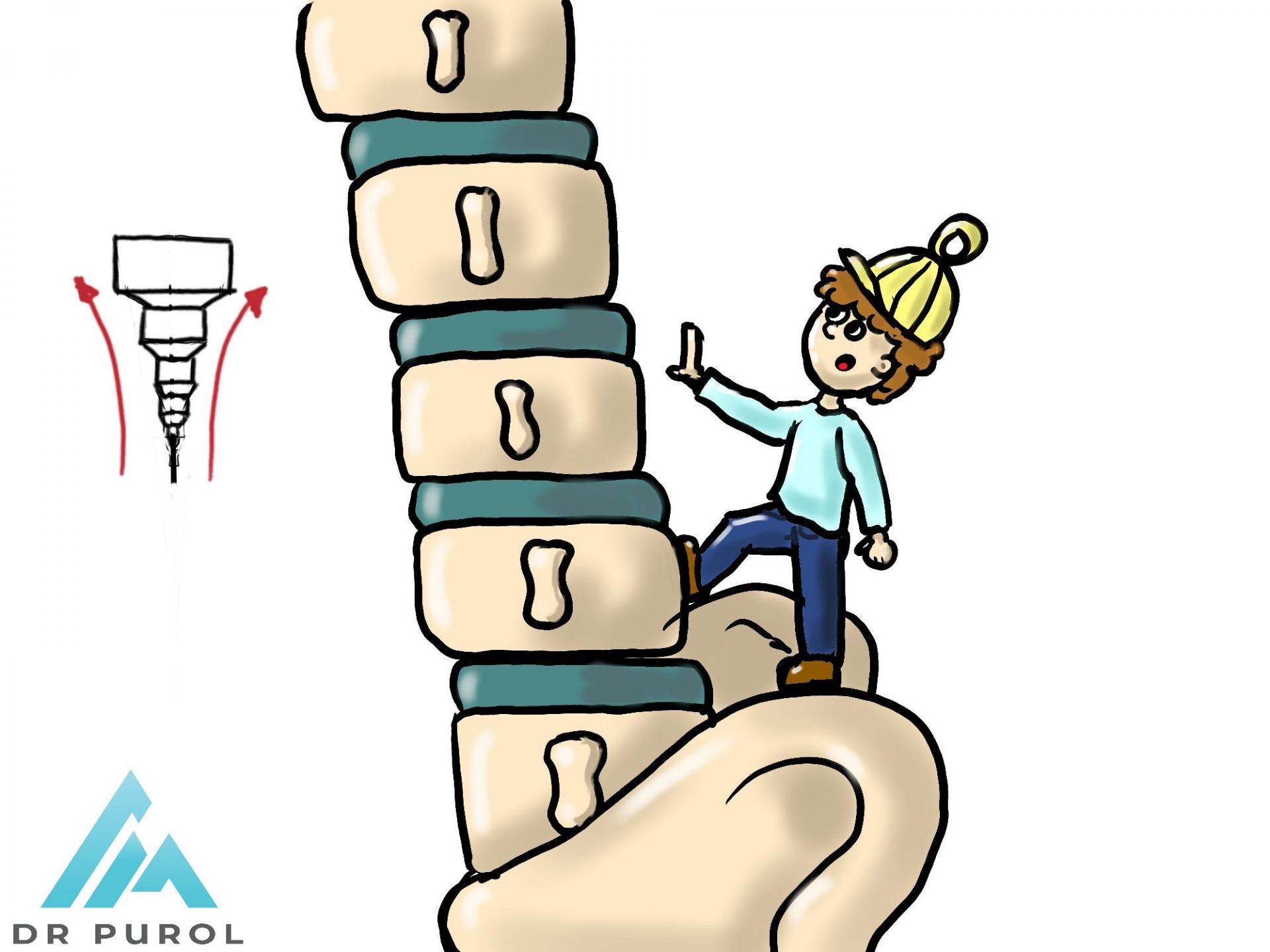
- and disorders of the physiological thoracic kyphosis or the sagittal lumbar lordosis


Remember! Any postural defect may accompany scoliosis and requires orthopedic evaluation to rule it out.
How do we diagnose scoliosis?
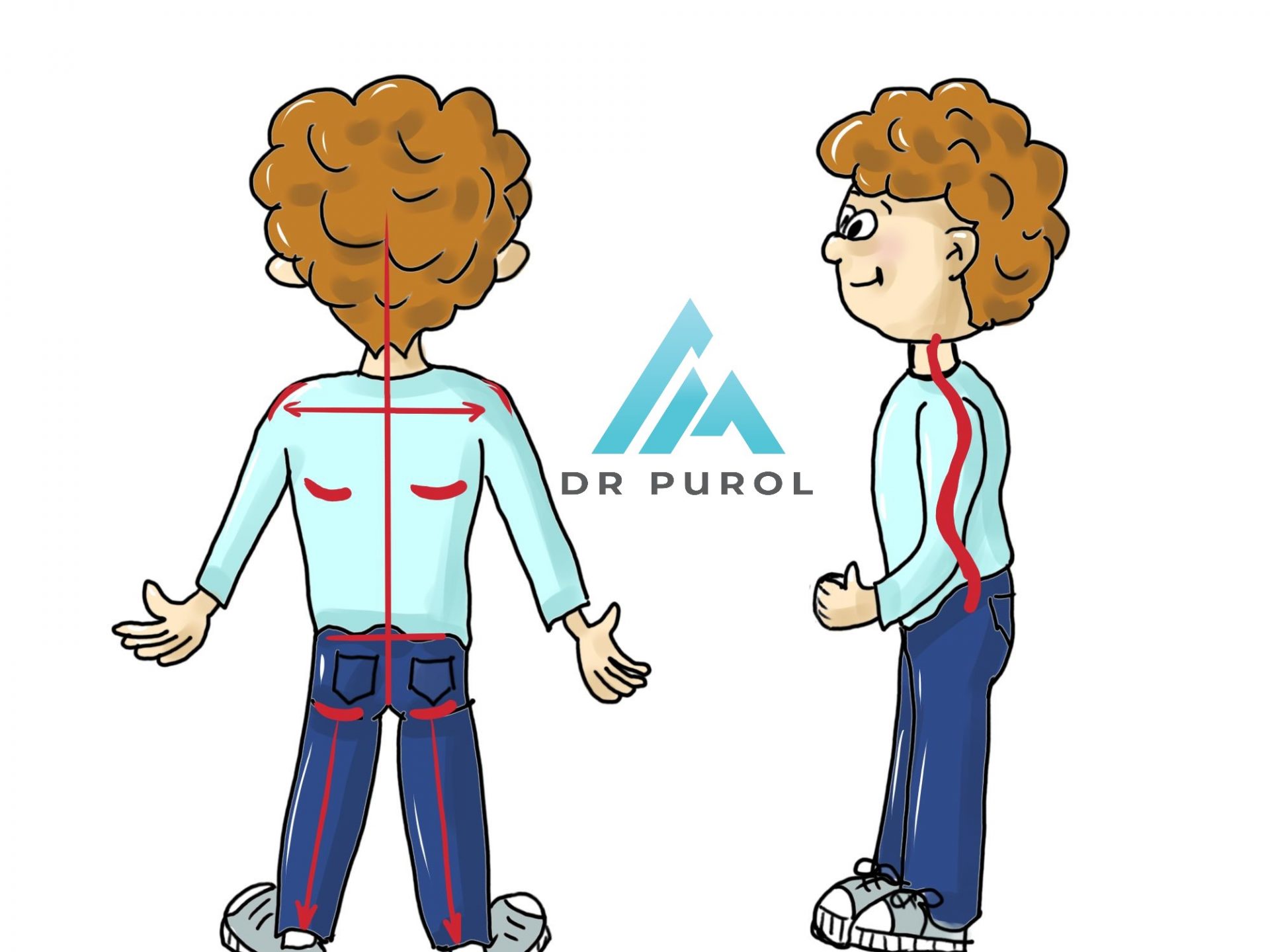
The torso assessment begins with a clinical examination of the torso. We assess the symmetry of the shoulders, shoulder blades, waist, pelvis position, and check the length of the lower limbs. Then we examine the spine – standing behind the patient – we check for any side curvatures and standing from the side of the patient, we assess our natural curves, i.e. cervical lordosis, thoracic kyphosis and lumbar lordosis.

In the next stage, we ask you to perform the Adams test, which means a forward bend – this test perfectly differentiates scoliosis from posture defects. First, postural defects do not lead to spine rotation, so they do not cause asymmetry in the form of costal humps or lumbar shafts present in scoliosis. Second, the functional curvature in the test is fully straightened, while in structural scoliosis, the spine will still resemble the letter “C” or “S”.
What is a Scoliometer?
A scoliometer is a clinical examination support tool for detecting spinal rotation, which is considered to be the first stage of scoliosis. The norm is 0-3 degrees of deviation. Above 7 degrees, we diagnose scoliosis.
Is an x-ray always necessary?
YES, it is the basis for diagnosis. It allows us to control the possible progression of the curvature and the progress of the treatment. We select one of the possible treatment methods depending on the size of the curvature assessed in the photo. The x-ray photo also allows you to assess the child’s bone maturity (Risser test), which is important in prognostication.
How do we treat scoliosis?
Minor curvatures in the range of 10-24 degrees are treated with exercises, self-control of posture and generally understood physical activity. Never release your child from PE because of scoliosis !!
Larger deformities 25-40 in developmental age – corrective corsets, usually used around the clock for several months. The success of corset treatment is to stop the curvature progression.
Major curvatures above 45 degrees require surgical treatment.
text author: Maciej
drawings: Agnieszka